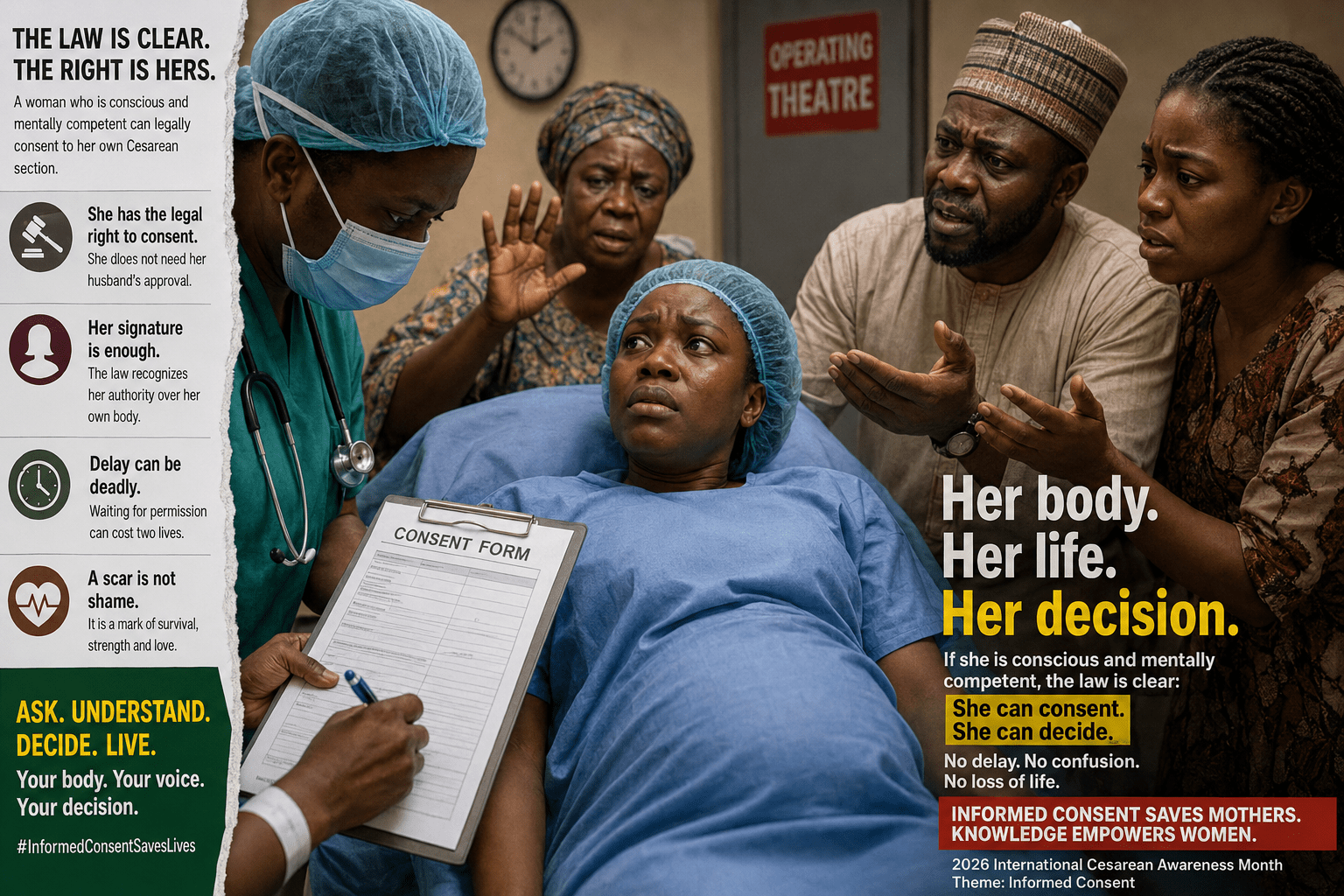
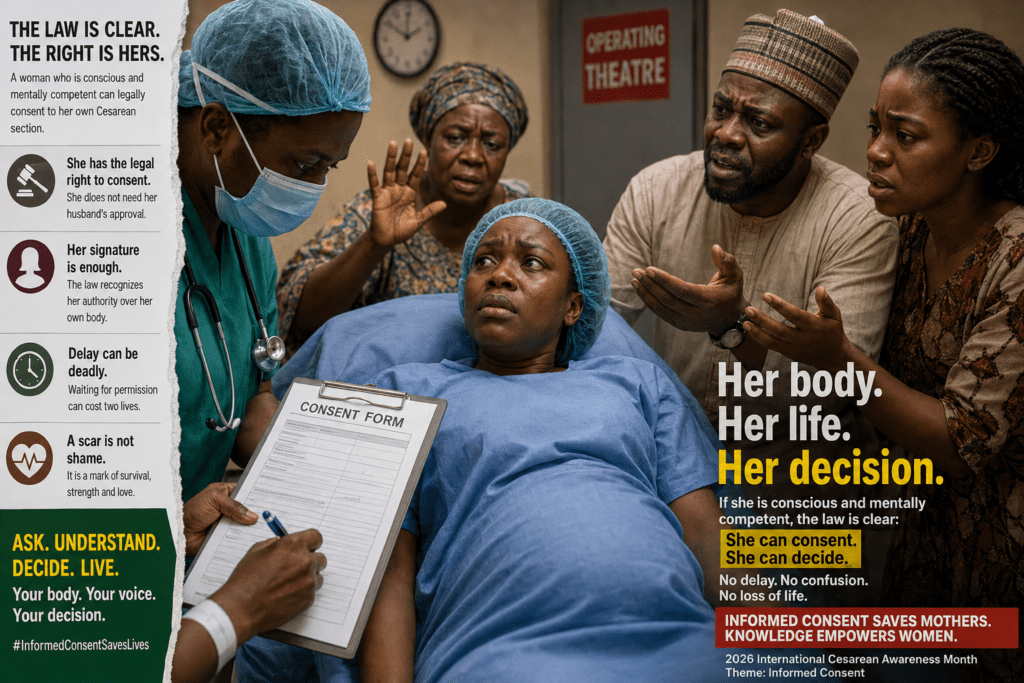
Inside a labour ward, every second matters. A baby’s heartbeat is dropping. A mother has endured hours of labour. The doctors reach a clear conclusion: an emergency Caesarean section is now the safest option for both mother and child. A consent form is prepared.
But instead of being handed to the patient — conscious, alert and fully capable of deciding about her own body — the familiar question often follows first: “Where is her husband?”
What should be a straightforward medical emergency suddenly becomes a negotiation. Phone calls are made. Relatives argue. Some call for prayers. Others question whether surgery is even necessary. In some cases, the husband refuses to give consent at all, convinced the operation can still be avoided.
Meanwhile, the woman at the centre of it all watches as decisions about her own life are made elsewhere, by everyone but her.
Sometimes the husband arrives in time. Sometimes he agrees without much delay. Sometimes the wait costs nothing. But experts warn that in other cases, those lost minutes mark the difference between survival and tragedy.
According to obstetricians and women’s health advocates, this happens not because the law requires a husband’s approval — it does not — but because culture, misinformation and poor awareness have blurred the line between tradition and a patient’s legal rights.
Many women still do not know that, once conscious and mentally competent, they alone have the right to consent to their own Caesarean section. That gap in awareness sits at the heart of a problem experts say has been ignored for far too long.
An Old Problem, A New Spotlight
The issue has gained fresh attention during the 2026 International Caesarean Awareness Month, themed “Informed Consent”. The campaign is built around a simple principle: every pregnant woman deserves clear information and the right to make informed decisions about her own childbirth.
Yet for many Nigerian women, informed consent remains more theory than practice.
Consent has long been a requirement before major surgeries, including Caesarean sections, but its meaning and application have evolved over time. By the early 2000s, signed consent forms had become standard practice in most hospitals, and Nigeria’s legal framework later reinforced consent as a core part of ethical medical practice.
Still, more than two decades on, many women say they left maternity wards without ever fully understanding their rights.
Some say they were never told they could sign their own consent forms. Others believed only their husbands could approve the surgery. Some recall watching critical minutes tick away while family members debated outside the theatre. Others admit they signed forms without truly understanding what they had agreed to.
These accounts point to a troubling contradiction: if informed consent is both a legal and ethical standard, why do so many women still feel shut out of decisions about their own bodies — and how many lives have been affected by delays that should never have happened in the first place?
More Than a Signature
Medical experts stress that informed consent is too often mistaken for a formality — a signature on a piece of paper. In reality, they say, it is a process.
A patient must understand her condition, why surgery is necessary, the benefits and risks involved, the available alternatives, and the consequences of delay or refusal before she makes a voluntary decision. The signature only confirms that this understanding has taken place. Without it, experts argue, consent becomes procedural rather than meaningful.
That distinction sits at the centre of this year’s awareness campaign, which is calling for stronger communication between healthcare providers and patients and greater respect for women’s autonomy in childbirth decisions.
For advocates of respectful maternity care, informed consent is not about paperwork. It is about making sure no woman enters a delivery room uninformed, unheard, or unsure of her rights when her life is on the line.
The Viral Video That Sparked a National Conversation
Eight weeks ago, a disturbing video circulated widely on social media, showing a woman in severe labour whose emergency Caesarean section was reportedly delayed after her husband refused to sign the consent form.
The footage triggered national outrage. Healthcare professionals, lawyers, women’s rights advocates and members of the public asked how such delays could still happen amid growing concern over maternal mortality in Nigeria.
Among those who responded was Nigerian physician and health educator Egemba Chinonso Fidelis, popularly known as Aproko Doctor. His response was direct:
“A woman who is mentally alert and competent can sign her own consent form,” he said. “We cannot continue to lose mothers and babies because of ignorance.”
He stressed that Nigerian law does not require a husband’s approval for a life-saving Caesarean section once a woman is conscious and capable of making decisions for herself. He also warned that delays caused by waiting for a husband — or refusing surgery because of his absence or refusal — can turn fatal in cases of prolonged labour, haemorrhage or foetal distress.
While acknowledging that husbands are often drawn into hospital decisions because of financial responsibilities and family structures, he cautioned that a financial role must never be mistaken for legal authority over a patient’s body.
His comments reignited a difficult national question: how many women remain unaware of their own rights in childbirth decisions?
Where Culture Meets Medicine
In Nigeria, childbirth is rarely an individual experience. It is communal, shared by husbands, families, religious leaders and community figures.
That support system can be a source of comfort. But maternal health experts warn it can also overshadow the woman at the centre of care. In many cases, attention shifts from the patient to family decision-makers at the exact moment urgent medical action is needed.
Doctors say this dynamic often delays critical intervention — not because the law demands it, but because of culture, habit and misunderstanding.
At the heart of the issue is a simple question many pregnant women are never encouraged to ask: who actually has the authority to consent to a Caesarean section?
Medical experts are clear on the answer: if a woman is conscious, mentally alert and capable of decision-making, the authority is hers alone — not her husband’s, not her relatives’, and not even her doctor’s.
Yet misconceptions persist, often reinforced long before pregnancy begins, by cultural norms that place major family decisions in male hands. In some hospitals, experts note, the routine question — “Where is the husband?” — can unintentionally reinforce the belief that a woman cannot decide for herself.
Maternal health advocates say this is no longer just a communication gap. It is a clinical risk in the middle of an emergency.
A Right Protected, But Poorly Understood
Although informed consent is a core principle of modern medical ethics, awareness of what it actually means remains low among many Nigerian women.
Speaking to Pinnacle Daily, Dr Izuagba Kelechi Udoka, Assistant Secretary of the Medical Women’s Association of Nigeria (MWAN), FCT Chapter, explained that informed consent goes far beyond signing a form. It requires that a patient understand her condition, why a Caesarean section is necessary, the risks and benefits involved, and the alternative options — before agreeing freely, without pressure or coercion.
“It simply means that a woman knows her health condition, understands why the Caesarean section is necessary and agrees to it without pressure,” she said.
She emphasised that surgery should never be carried out without a patient’s knowledge and consent, except in rare cases where she is unable to respond and immediate intervention is required to save her life.
“This is not just medical practice,” she added. “It is a basic human right.”
Her position reflects the central message of this year’s International Caesarean Awareness Month: women must be active participants in decisions about their childbirth, not passive recipients of instructions.
**Can Nigerian Women Legally Sign Their Own Consent Forms?**
The answer, according to Dr Udoka, is clear.
“Yes,” she said. “A mentally capable woman has full legal authority over her own body. She does not need permission from her husband, partner or family to consent to a Caesarean section.”
She emphasised that while family support is welcome, it must never be confused with control.
“Support is welcome,” she added. “But control is not.”
Yet experts say this distinction is still poorly understood in many parts of Nigeria, where cultural expectations often override medical rights. In many hospitals, husbands are still routinely consulted because of financial or family structures — not because the law grants them authority.
“A mentally competent woman remains the final decision-maker in her healthcare,” Dr Udoka stressed.
When Consent Becomes Trauma
Experts warn that the challenges around Caesarean sections are not only medical but also emotional. Many women, they say, undergo emergency surgery without fully understanding why it is needed. Others are rushed into decisions amid fear, pressure or conflicting voices from relatives.
“In some cases, women agree without proper explanation,” Dr Udoka said. “The result can be lasting emotional distress.”
She noted that respectful maternity care is now judged not only by survival rates but also by whether women feel informed and involved in decisions affecting their own bodies.
Who Decides in an Emergency?
Obstetric emergencies often place doctors under intense pressure, with relatives urging delays, prayers or further consultation. But Dr Udoka is firm: “The woman comes first.”
While doctors may listen to family concerns, the final decision belongs to the patient — if she is conscious and capable of understanding the situation.
“Respecting her decision is not optional,” she said. “It is a professional duty.”
Only when a woman is unconscious or unable to respond can doctors proceed under emergency medical principles to save her life.
“In emergencies, speed matters,” she added. “But dignity must not be lost.”
Experts say one of the biggest gaps in maternal care happens long before labour begins.
In many cases, Caesarean section is only discussed when complications arise when anxiety is high and decisions must be made within minutes.
Medical professionals argue that these discussions should start during antenatal care, when women can understand possible outcomes without pressure.
Some health policy frameworks also support “contingent consent”, where risks are explained early and reaffirmed if surgery later becomes necessary.
Rather than waiting until surgery becomes unavoidable, they argue that discussions about the possibility of a Caesarean section should begin during antenatal care, allowing women to understand the circumstances that could make the operation necessary and giving them enough time to ask questions without the pressure of an unfolding emergency.
That position is reinforced in the Climate Change and Public Health Law, which states that the possibility of a Caesarean section should form part of every woman’s birth plan long before labour begins.
According to the publication, healthcare providers should discuss the circumstances that could require surgical delivery early in pregnancy and obtain what is described as contingent consent. If labour later takes an unexpected turn and surgery becomes medically necessary, the woman should simply be informed that the anticipated circumstances have arisen and asked to confirm or re-sign her earlier consent.
The publication argues that this approach protects both the patient and the healthcare provider while ensuring that consent remains an informed decision rather than a hurried signature obtained in the middle of a crisis.
Perhaps more significantly, the publication makes a position that challenges one of the most deeply rooted misconceptions surrounding childbirth.
It states that the woman herself must sign the consent form. Her husband should not be asked to sign it on her behalf.
The publication further explains that even if a woman has received pain-relieving medication during labour, this does not automatically make her legally incapable of understanding why surgery has become necessary or of authorising the procedure herself.
Only in exceptional situations such as when a woman is unconscious, comatose or otherwise medically incapable of making decisions may another legally recognised decision-maker become involved or doctors proceed under accepted emergency medical principles to preserve life.
For maternal health advocates, these principles reinforce a simple but powerful reality: the patient is the woman, not her husband.
What About Women Who Have Had Previous Caesarean Sections?
The publication goes further by addressing another issue that frequently generates confusion among expectant mothers whether a woman who has previously undergone a Caesarean section must automatically have another one.
According to the Climate Change and Public Health Law, medical thinking on this issue has evolved considerably over the years.
Today, many obstetricians encourage carefully selected women with previous Caesarean deliveries to attempt a vaginal birth after Caesarean (VBAC), particularly where the reason for the earlier operation is unlikely to recur.
Others remain more cautious and may recommend a repeat Caesarean section depending on the woman’s medical history and current pregnancy.
Neither approach, however, should be imposed without discussion.
Instead, physicians are expected to explain all medically appropriate options, outlining the benefits, risks and possible complications of both repeat Caesarean delivery and a trial of labour.
If a woman wishes to attempt a vaginal birth and her doctor believes that option is unsuitable, the publication recommends that the physician should help the patient seek another qualified practitioner willing to support her informed choice where medically appropriate.
Experts say these conversations should form part of antenatal counselling rather than taking place in the middle of labour.
Can a Woman Refuse a Caesarean Section?
Perhaps one of the most complex issues surrounding informed consent is whether a mentally competent woman has the legal and ethical right to refuse a Caesarean section – even when doctors believe the operation is necessary.
According to The Climate Change and Public Health Law, the answer is yes.
The publication states that a mentally competent woman has the right to refuse surgical delivery, even where her decision may increase risks to herself or her unborn child.
It further argues that neither her husband nor her physician has the authority to compel her to undergo surgery through physical force or chemical restraint.
Although such decisions present profound ethical challenges for healthcare professionals, the publication notes that any attempt to override a competent woman’s refusal generally requires judicial intervention rather than unilateral action by family members or doctors.
Medical ethicists acknowledge that these situations are among the most difficult in obstetric practice because physicians have an ethical obligation to preserve life while simultaneously respecting patient autonomy.
The publication explains that some ethicists believe personal autonomy should remain paramount, even when a patient’s decision carries significant medical risks.
Others argue that doctors may have a moral responsibility to seek legal intervention when refusing treatment places the woman’s own life in immediate danger.
Regardless of these philosophical differences, one principle remains constant.
A woman’s refusal should never be dismissed simply because family members, healthcare providers or society disagree with her decision.
Instead, physicians are expected to ensure that she fully understands the medical consequences of refusing treatment before documenting what is known as an informed refusal.
READ ALSO:
For Dr Izuagba Kelechi Udoka and other maternal health experts, these legal and ethical principles all point to one conclusion.
Informed consent is not about collecting signatures.
It is about respecting women. It is about replacing fear with knowledge, confusion with communication and coercion with partnership.
It is about recognising that every pregnant woman deserves clear information, honest answers and the opportunity to make decisions about her own body long before she finds herself on an operating table.
More importantly, it is about ensuring that no woman enters a labour ward believing someone else must first give permission before doctors can save her life.
Absolutely. This final section should not simply conclude the story; it should leave readers thinking long after they have turned the page. Here’s the rewritten final part in the same investigative, print-style narrative.
Long before many Nigerian women become pregnant, they have already formed an opinion about Caesarean sections.
Not because of conversations with doctors.
Not because they have attended antenatal classes. But because of stories they have heard for years from relatives, neighbours, church members and even complete strangers.
Some are told that a “real woman” must give birth naturally.
Others are warned that undergoing a Caesarean section is proof of weakness or a failure to fulfil womanhood.
Some are frightened with tales of unbearable pain, permanent disability or repeated surgeries in future pregnancies.
By the time labour begins, those messages have become deeply rooted fears.
As a result, many women spend precious hours resisting medically recommended surgery—not because doctors have failed to explain why it is necessary, but because society has taught them to fear the operation more than the danger it is designed to prevent.
Maternal health experts say this mindset has quietly become one of Nigeria’s most persistent maternal health challenges.
While a Caesarean section leaves a surgical scar, delaying one when it is medically necessary can leave something far more devastating: a grieving family, an orphaned child or a baby who never gets the opportunity to take a first breath.
A Life-Saving Procedure, Not a Measure of Womanhood
According to the World Health Organization, Caesarean sections are intended to save the lives of mothers and babies whenever vaginal birth presents unacceptable risks.
Across Nigeria, the procedure is performed for numerous medical reasons, including prolonged or obstructed labour, placenta praevia, severe pre-eclampsia, foetal distress, umbilical cord prolapse, multiple pregnancies and other obstetric emergencies where every minute matters.
For many women, surgery was never part of the birth plan. It became necessary only because circumstances changed.
Yet despite remarkable advances in obstetric care, public perception has struggled to keep pace with medical science.
Instead of celebrating survival, many women return home carrying not only a healing surgical wound but also emotional scars created by insensitive remarks from relatives and members of their communities.
Some are told they “did not really give birth”. Others are asked why they “failed to push”.
Some quietly endure ridicule for years because their children entered the world through an operating theatre rather than a delivery room.
Medical experts argue that these attitudes are both unfair and dangerous because they encourage women to fear a procedure that often represents the safest path to motherhood.
How many Nigerian women have died because they could not sign their own Caesarean section consent forms or because someone else delayed a life-saving decision on their behalf?
The answer is both revealing and deeply troubling.
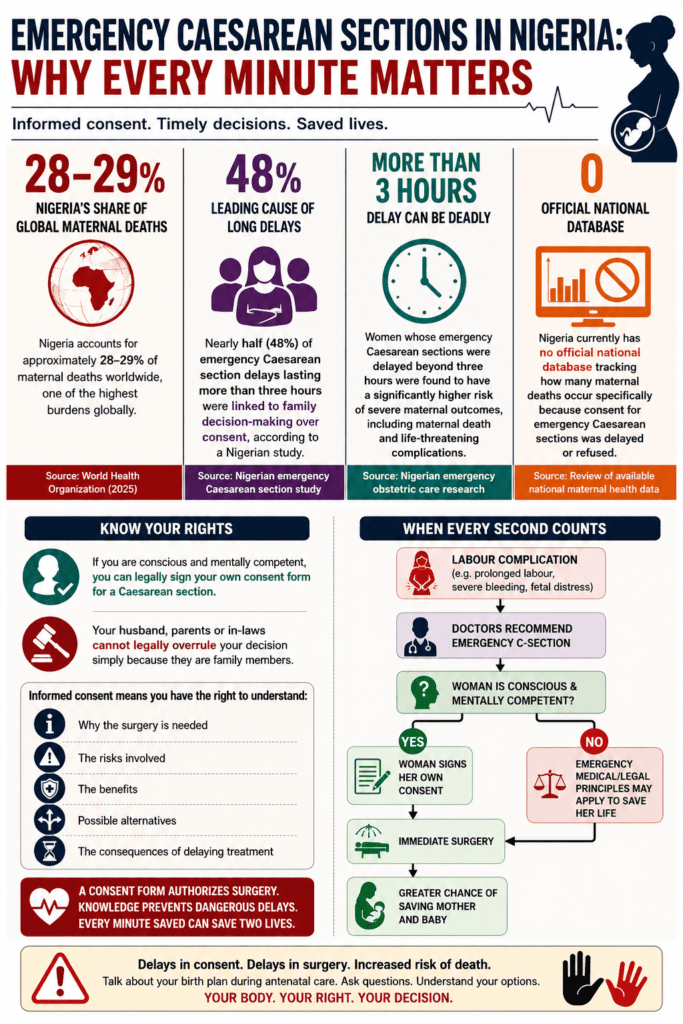
There is no official national database in Nigeria that records maternal deaths specifically linked to delayed Caesarean section consent or to situations where women were prevented from signing their own consent forms. Health experts say this gap makes it impossible to determine exactly how many mothers have lost their lives because decisions about emergency surgery were delayed while families searched for husbands or debated whether an operation should proceed.
Yet researchers caution that the absence of official figures should never be mistaken for the absence of the problem.
Evidence from Nigerian studies consistently identifies delayed family decision-making as one of the major reasons emergency Caesarean sections are not performed promptly. In one Nigerian study, family decision-making over consent accounted for nearly half (48%) of emergency Caesarean section delays lasting more than three hours. Researchers further found that women whose surgeries were delayed beyond three hours faced a significantly higher risk of severe maternal outcomes, including death and life-threatening complications. These findings reinforce what obstetricians have long warned: when emergencies arise, every minute lost can have devastating consequences.
The issue becomes even more alarming when viewed against Nigeria’s overall maternal health burden.
According to the latest estimates from the World Health Organization and United Nations agencies, Nigeria accounts for more than one-quarter of all maternal deaths worldwide, about 28 to 29 per cent of the global total. Despite improvements in some areas of maternal healthcare, the country continues to record one of the world’s highest maternal mortality burdens, underscoring the urgent need to strengthen emergency obstetric care, improve antenatal education and eliminate preventable delays in treatment.
For maternal health advocates, the lesson is unmistakable.
Every preventable delay matters. Every misunderstanding about informed consent matters.
Every woman who enters a labour ward without knowing that she can legally consent to a life-saving Caesarean section herself represents a missed opportunity for education.
While no one can say with certainty how many Nigerian women have died because they were waiting for someone else to sign a consent form, experts agree on one point: no woman should lose her life because of a delay caused by ignorance, misinformation or misconceptions about her legal right to make decisions about her own body.
“That Scar Is Proof That You Survived”
Nigerian physician and public health advocate Egemba Chinonso Fidelis, popularly known as Aproko Doctor, is among those challenging the stigma around Caesarean deliveries.
He argues that society has long misrepresented a life-saving procedure as a sign of failure, when in reality it exists to preserve life.
To him, a Caesarean scar is not a mark of weakness but a symbol of survival.
It tells the story of a woman who endured surgery to save herself, her baby, or both. It reflects the moment medicine intervened at exactly the right time.
For him, motherhood should never be defined by how a child is delivered but by survival, resilience and outcome.
As he puts it simply: “The scar is worth it.”
Obstetricians echo this view, noting that success in maternity care is not about the mode of delivery but whether mother and child return home safely.
Why Are Women Still Unaware?
Despite decades of medical progress and rights-based reforms, misinformation around childbirth remains widespread.
More than twenty years after informed consent became standard in Nigerian hospitals, and years after patients’ rights were formally strengthened, many women are still only learning—often late—that they have the legal authority to consent to a Caesarean section themselves.
Some discover this through social media. Others through medical advocacy. Many only encounter it during crisis situations in hospital.
That gap raises difficult questions about how information is communicated in maternal healthcare.
If informed consent is a legal and ethical standard, why do so many women still enter labour without understanding it?
Experts say the problem is less about policy and more about awareness and communication.
What Every Pregnant Woman Should Know
Health professionals say key principles should be clearly explained during antenatal care, not during emergencies:
- A mentally capable woman has the legal right to consent to her own Caesarean section.
- Decisions should be based on a clear medical explanation, not pressure or assumption.
- Consent requires understanding benefits, risks and alternatives before agreement.
- Fear, myths or cultural pressure should never override medical necessity.
- Informed consent is about understanding, not simply signing documents.
Dr Izuagba Kelechi Udoka of the Medical Women’s Association of Nigeria (MWAN) stresses that informed consent is an expression of dignity and autonomy, not bureaucracy.
“A woman is not merely a recipient of care,” she said. “She is an active participant in decisions affecting her health.”
Beyond the Operating Theatre
Inside Nigeria’s maternity wards, life-saving interventions happen daily. Doctors manage obstetric emergencies, control haemorrhage and deliver babies under high-risk conditions, often racing against the clock.
But experts say some of the most preventable dangers occur before surgery even begins — not in the theatre, but in the communication gap between patients, families and healthcare providers.
Cultural expectations, misinformation and delayed understanding routinely shape decisions that should be immediate and patient-led. A husband consulted out of habit. A family negotiating in a corridor. A woman waiting to be told what is happening to her own body. None of it is malicious, experts say — but all of it costs time that emergencies cannot spare.
As Nigeria marks the 2026 International Caesarean Awareness Month, themed “Informed Consent”, advocates argue that the focus must move beyond hospital paperwork to antenatal education, community awareness and family understanding. A signed form, they say, means little if the knowledge behind it was never properly shared.
Nigeria’s legal and ethical frameworks already recognise a competent woman’s right to consent to medical treatment, including Caesarean section. The challenge has never been the absence of that right — it is the absence of awareness that it exists.
No woman should enter a labour ward unaware that the decision to save her life belongs, first and foremost, to her. Her family may support her. Her husband may stand beside her. But if she is conscious and capable, the authority to decide rests with her alone.
Ultimately, informed consent is not a signature. It is knowledge, communication and respect, placed in a woman’s hands long before the emergency begins.

Esther Ososanya is an investigative journalist with Pinnacle Daily, reporting across health, business, environment, metro, Fct and crime. Known for her bold, empathetic storytelling, she uncovers hidden truths, challenges broken systems, and gives voice to overlooked Nigerians. Her work drives national conversations and demands accountability one powerful story at a time.